ABO Blood Group Genetics — Alleles, Antigens, and Codominance
The ABO blood group system is one of the most clinically significant genetic traits in humans. Karl Landsteiner discovered it in 1901, winning the Nobel Prize in Physiology or Medicine in 1930. The system is controlled by the ABO gene on chromosome 9q34, which encodes a glycosyltransferase enzyme that modifies the H antigen on red blood cell surfaces.
Three functional alleles exist at this locus. The IA allele encodes A-N-acetylgalactosaminyltransferase, which adds N-acetylgalactosamine to the H antigen, producing the A antigen. The IB allele encodes A-galactosyltransferase, which adds D-galactose to produce the B antigen. The i allele encodes a non-functional enzyme that leaves the H antigen unmodified — producing neither A nor B antigens, giving blood type O.
IA and IB are codominant — both enzymes function independently in the same cell, so a person with genotype IAIBexpresses both A and B antigens simultaneously, producing blood type AB. This is a textbook example of codominance in genetics. The i allele is recessive to both IA and IB.
| Blood Type | Possible Genotypes | Antigens on Red Cells | Antibodies in Plasma | Frequency (European) |
|---|---|---|---|---|
| A | I^A I^A or I^A i | A antigen | Anti-B | ~42% |
| B | I^B I^B or I^B i | B antigen | Anti-A | ~10% |
| AB | I^A I^B | A and B antigens | Neither (universal recipient) | ~4% |
| O | ii | None (H antigen only) | Anti-A and Anti-B | ~44% |
Rh Factor Inheritance and Rh Incompatibility in Pregnancy
The Rh blood group system is the second most clinically important blood group after ABO. It comprises over 50 antigens, but the D antigen is by far the most significant. The presence of the D antigen on red blood cells defines an individual as Rh-positive (Rh+); its absence defines Rh-negative (Rh−).
Rh factor is controlled by the RHD gene on chromosome 1p36. The D allele (Rh+) is dominant over the d allele (Rh−). Rh+ individuals are either homozygous (DD) or heterozygous (Dd). Rh− individuals are homozygous recessive (dd). Because Rh+ heterozygotes (Dd) are phenotypically identical to homozygotes (DD), two Rh+ parents can produce Rh− children — approximately 25% of offspring if both parents are Dd.
Rh Incompatibility — Clinical Significance
When an Rh− mother carries an Rh+ foetus, foetal red blood cells can cross into the maternal circulation — most commonly during delivery, but also during miscarriage, amniocentesis, or trauma. The mother's immune system may produce anti-D IgG antibodies (alloimmunisation).
In subsequent Rh+ pregnancies, these anti-D antibodies cross the placenta and destroy foetal red blood cells, causing haemolytic disease of the foetus and newborn (HDFN). Severe HDFN causes anaemia, hyperbilirubinaemia, kernicterus, hydrops fetalis, and can be fatal without intervention.
Prevention: Anti-D immunoglobulin (RhoGAM) given to Rh− mothers at 28 weeks gestation and within 72 hours of delivery prevents alloimmunisation in the vast majority of cases. This is one of the most successful prophylactic interventions in obstetric medicine.
Worked Blood Type Inheritance Examples
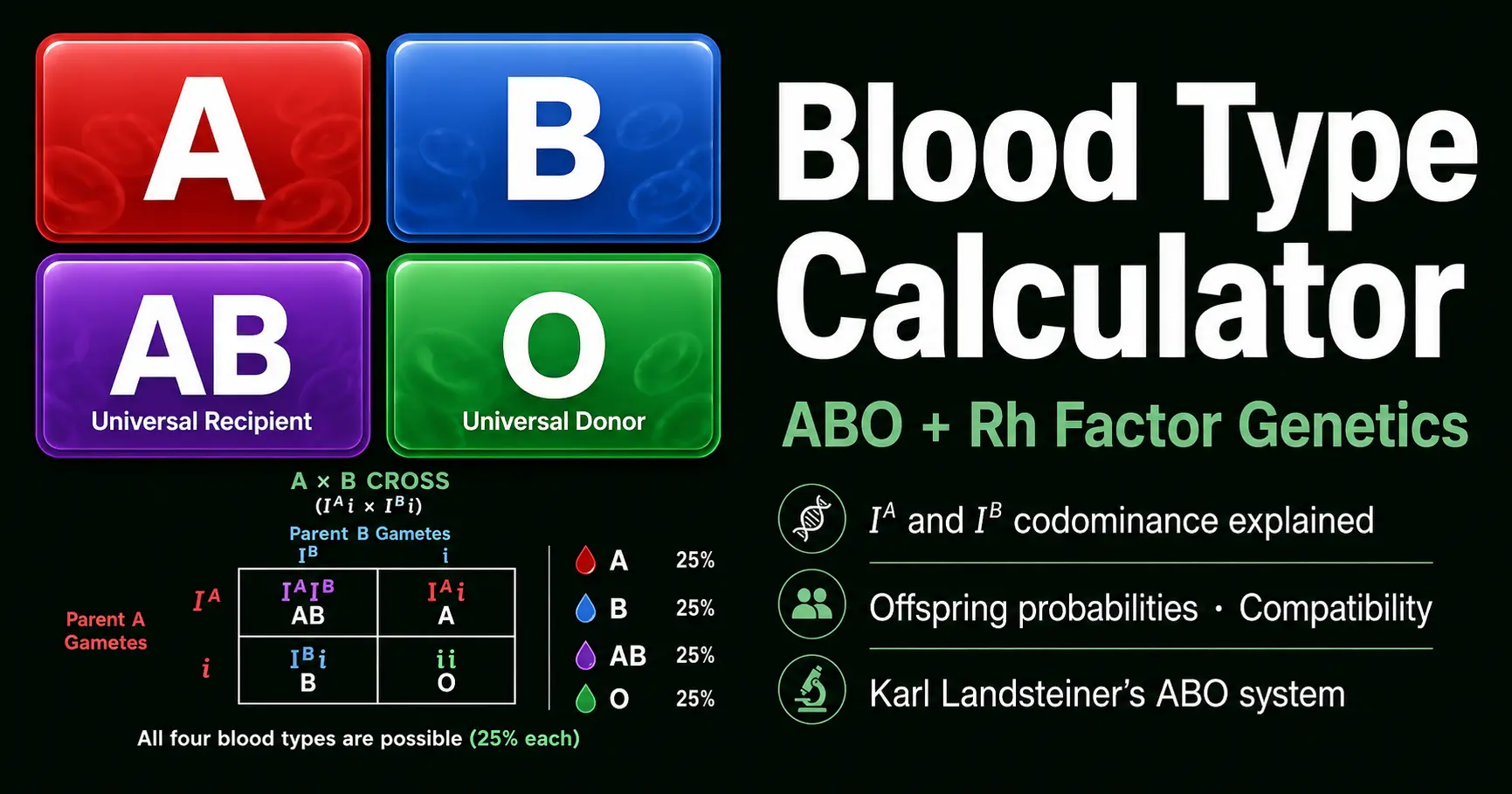
Example 1 — A × B: All four blood types possible
When one parent is type A (IAi) and the other is type B (IBi), all four blood types are possible in offspring. This is the only parental combination that can produce A, B, AB, and O children.
Example 2 — O × O: Only type O offspring
Two type O parents are both genotype ii. They can only pass on the i allele. Every child will be ii — blood type O. No exceptions.
Example 3 — AB × O: A and B only
An AB parent (IAIB) crossed with an O parent (ii) produces only A and B children — never AB or O. This is because the AB parent cannot pass on the i allele, and the O parent cannot pass on IAor IB.
Blood Type Transfusion Compatibility Chart
ABO and Rh compatibility is critical in blood transfusions. Receiving incompatible blood triggers an acute haemolytic transfusion reaction — the recipient's pre-formed antibodies attack the transfused red cells, causing rapid haemolysis, renal failure, and potentially death. The WHO Blood Transfusion Safety guidelines mandate ABO and Rh compatibility testing before every transfusion.
| Blood Type | Can Donate Red Cells To | Can Receive Red Cells From |
|---|---|---|
| O− | All types (universal donor) | O− only |
| O+ | O+, A+, B+, AB+ | O+, O− |
| A− | A+, A−, AB+, AB− | A−, O− |
| A+ | A+, AB+ | A+, A−, O+, O− |
| B− | B+, B−, AB+, AB− | B−, O− |
| B+ | B+, AB+ | B+, B−, O+, O− |
| AB− | AB+, AB− | A−, B−, AB−, O− |
| AB+ | AB+ only | All types (universal recipient) |
These rules apply to red blood cell transfusions. Plasma compatibility is reversed (AB is universal plasma donor). Platelet compatibility depends on both ABO and HLA matching.
Frequently Asked Questions — Blood Type Genetics
How is ABO blood type inherited from parents?
Can two O-type parents have an A or B child?
Can two AB parents have an O-type child?
How is Rh factor inherited?
What is haemolytic disease of the newborn caused by Rh incompatibility?
What does universal donor and universal recipient mean?
Can blood type determine paternity?
What blood types can donate to each other?
Related Tools
Baby Genetics Calculator
Predict eye colour, hair colour, and blood type probabilities together.
Open CalculatorCodominance Calculator
ABO blood typing is the classic codominance example — model any codominant cross.
Open CalculatorPunnett Square Calculator
Mendelian genetics crosses — monohybrid to pentahybrid with ratio analysis.
Open CalculatorHardy-Weinberg Calculator
Calculate ABO allele frequencies in a population under Hardy-Weinberg equilibrium.
Open Calculator