Genetic Disorders and Punnett Squares: Disease Risk
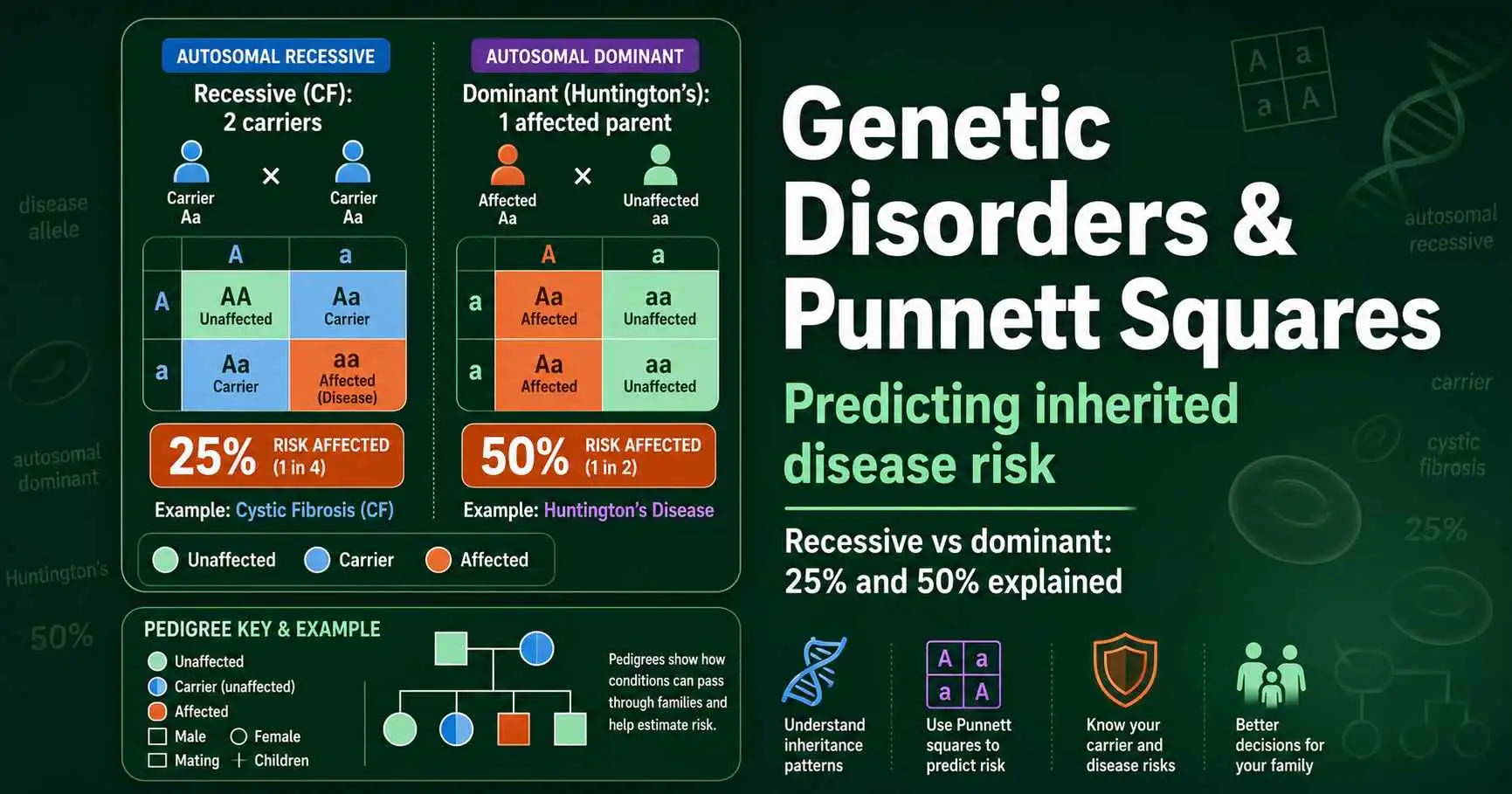
A Punnett square predicts the risk that a child inherits a genetic disorder, using the same method that works for any trait. The risk depends on the inheritance pattern. For an autosomal recessive disorder like cystic fibrosis, two carrier parents have a 25 percent chance of an affected child. For an autosomal dominant disorder like Huntington's disease, one affected parent gives each child a 50 percent chance. Knowing the pattern and the parents' genotypes lets you calculate the odds precisely.
Genetic counselors use exactly this reasoning every day to help families understand inherited risk. The math is the same Mendelian genetics you would use for pea plants, applied to conditions that matter deeply to real people. This guide explains the major inheritance patterns for genetic disorders, works through the key examples, and shows how a Punnett square turns a family history into a clear probability. If you want a refresher on carriers and the homozygous-versus-heterozygous distinction first, our guide on homozygous vs heterozygous genotypes sets the groundwork.
How Genetic Disorders Are Inherited
Most single-gene disorders follow one of three classic inheritance patterns, and identifying the pattern is the first step in predicting risk. The three classic patterns are autosomal recessive, autosomal dominant, and X-linked. Each behaves quite differently in a Punnett square, so naming the pattern tells you what odds to expect.
The word autosomal means the gene sits on one of the 22 non-sex chromosomes, so the disorder affects both males and females equally. Recessive means a person needs two copies of the disease allele to be affected, while dominant means a single copy is enough. X-linked means the gene sits on the X chromosome, which produces the sex-biased patterns where conditions strike one sex far more than the other. Most of this article focuses on the two autosomal patterns, since they are the most common and the clearest to predict.
The key variable in every case is the parents' genotypes. A disease allele can be present without being expressed, hiding in a carrier, so a parent's health does not always reveal what they carry. This is why genetic counseling often involves testing parents to learn their genotypes before estimating a child's risk. Once you know whether each parent is unaffected, a carrier, or affected, the Punnett square does the rest, converting genotypes into a precise probability of an affected child.
Autosomal Recessive Disorders: Cystic Fibrosis
Autosomal recessive disorders only appear when a person inherits two copies of the disease allele, one from each parent. Cystic fibrosis is the textbook example. It is caused by a mutation in the CFTR gene on chromosome 7, and a person develops the disease only with two copies of the faulty allele, the genotype often written as two lowercase letters.
The important figures in this group are carriers. A person with one normal allele and one disease allele is a heterozygous carrier. They are completely healthy, because their single normal allele produces enough working protein, but they carry the disease allele and can pass it on. Carriers are common in the population; roughly one in 30 people carries a cystic fibrosis allele without knowing it. A carrier shows no symptoms, which is exactly why these disorders can seem to appear out of nowhere in a family.
The risk arises when two carriers have children together. Each carrier parent has a 50 percent chance of passing the disease allele, so by the multiplication rule, there is a 50 percent times 50 percent, or 25 percent, chance that a child inherits two disease alleles and is affected. The same cross gives a 50 percent chance of a healthy carrier child and a 25 percent chance of a child with two normal alleles. This is the familiar 1:2:1 genotype ratio applied to disease, and it is the single most important pattern in this article.
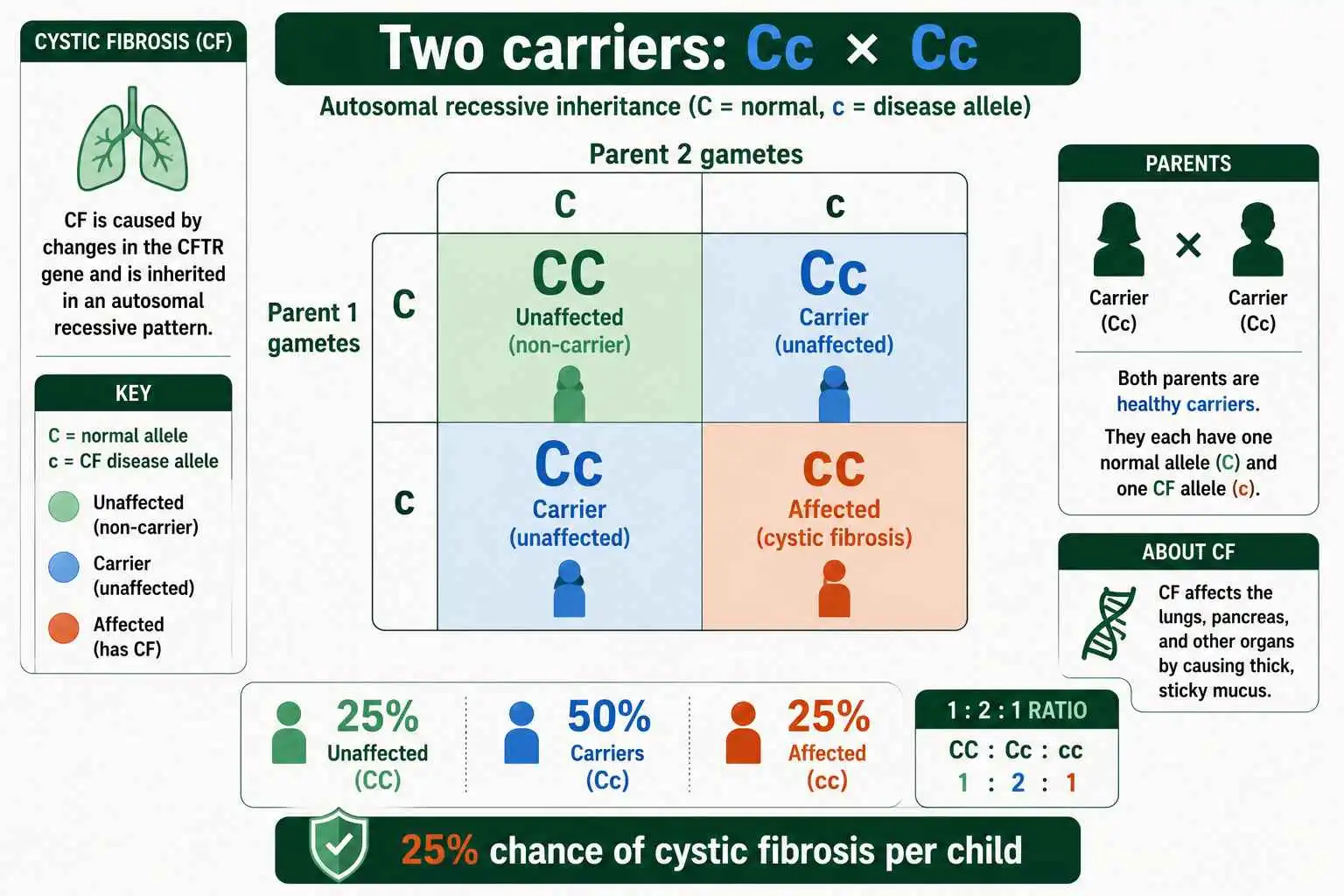
The Cystic Fibrosis Punnett Square
Setting up the cystic fibrosis cross uses a standard monohybrid square. Both carrier parents have the heterozygous genotype, with one normal allele and one disease allele. Each produces two kinds of gamete, one carrying the normal allele and one carrying the disease allele.
Filling the grid gives four equally likely outcomes: one child with two normal alleles, two children who are carriers, and one child with two disease alleles. Reading these by health status, three of the four children are unaffected, and one is affected with cystic fibrosis. That is the 25 percent risk, the same 3:1 healthy-to-affected ratio Mendel saw in pea plants, now describing a serious disorder.
The 25 percent figure applies to each pregnancy independently. A common misunderstanding is to think that if a couple has one affected child, their next three will be unaffected. That is not how probability works. Each child has the same 25 percent chance regardless of previous children, just as each coin flip is independent of the last. A couple could have several affected children in a row or none at all; the 25 percent is a per-child probability, not a quota. To estimate the precise odds for a given family situation, a carrier probability calculator applies this same logic to whatever genotypes the parents have.
Autosomal Dominant Disorders: Huntington's Disease
Autosomal dominant disorders work in the opposite way: a single copy of the disease allele is enough to cause the condition. Huntington's disease is the classic example, a progressive neurological disorder caused by a dominant allele. Because just one copy produces the disease, there is no healthy carrier state. If you have the allele, you will eventually develop the condition.
This changes the inheritance math considerably. An affected person is usually heterozygous, carrying one disease allele and one normal allele. When this person has children with an unaffected partner, each child has a 50 percent chance of inheriting the disease allele, and therefore a 50 percent chance of developing the disorder. The higher risk, 50 percent rather than 25 percent, is a hallmark of dominant disorders, since only one copy of the allele is needed.
Huntington's carries a poignant complication tied to its timing. Symptoms usually do not appear until a person is over 30 years old, often after they have already had children. This means a person can unknowingly pass the allele to their children before they themselves show any signs of the disease. The late onset is why Huntington's spreads through families in a way that earlier-onset conditions might not, and it is part of what makes genetic testing and counseling so significant for affected families.
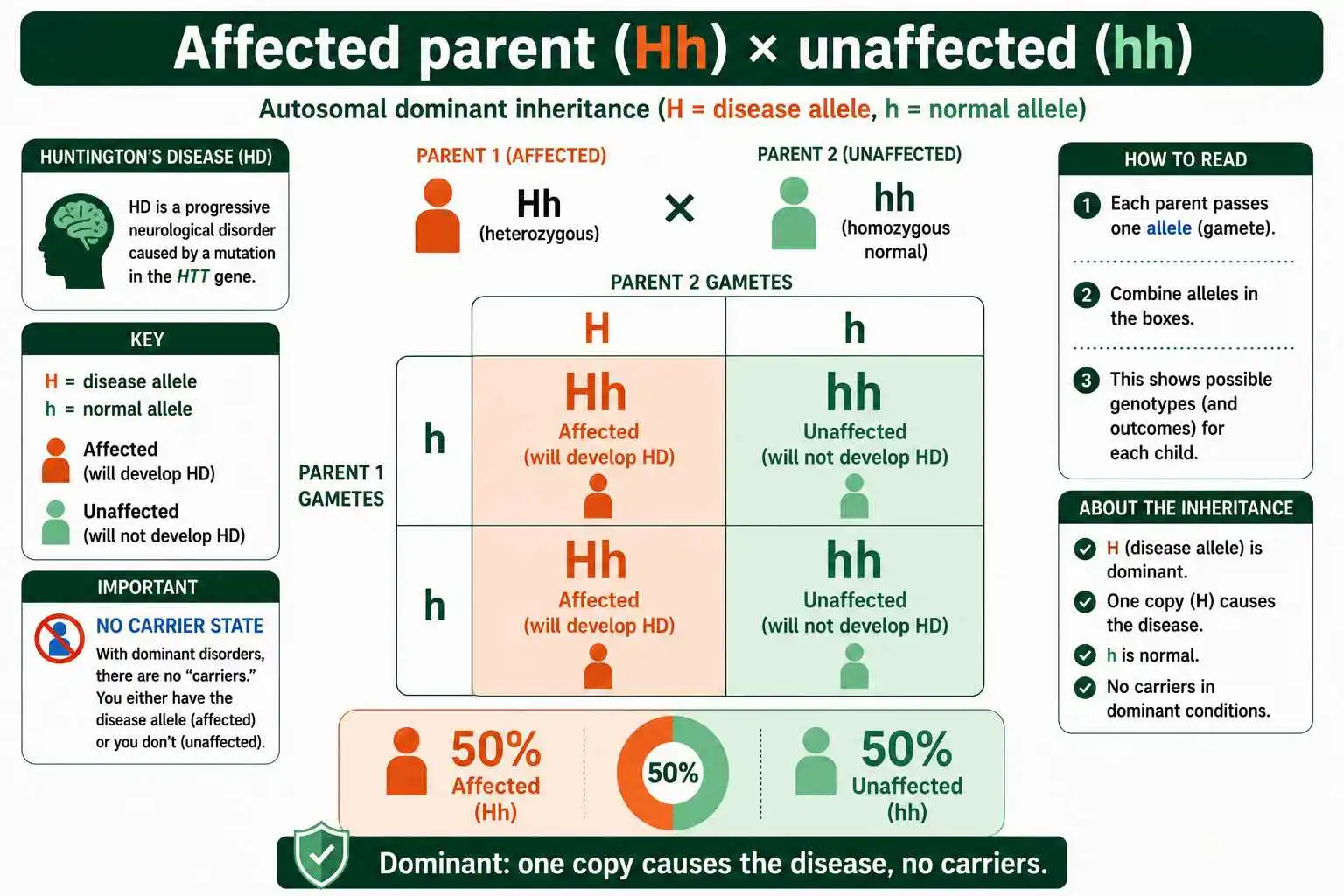
The Huntington's Disease Punnett Square
The Huntington's cross looks different from the cystic fibrosis one because the disease allele is dominant. The affected parent is heterozygous, carrying one dominant disease allele and one recessive normal allele. The unaffected parent has two normal recessive alleles.
When you fill the grid, the affected parent passes either the disease allele or the normal allele, while the unaffected parent can only pass a normal allele. The result is that half the children inherit the disease allele and half do not. Every child who inherits even one copy of the dominant disease allele will develop Huntington's, because no carrier state exists to shield them. So the cross gives a clean 50 percent risk for each child.
Comparing the two squares side by side reveals the core difference between recessive and dominant disorders. With a recessive disorder, two unaffected carriers produce a 25 percent risk, and the disease can hide for generations before appearing. With a dominant disorder, an affected parent produces a 50 percent risk, the condition appears in every generation, and there are no hidden carriers. Recognizing which pattern you are dealing with immediately tells you both the level of risk and how the disease moves through a family tree, which is why naming the inheritance pattern is always the starting point.
Sickle Cell Anemia: A Recessive Disorder With a Twist
Sickle cell anemia is another autosomal recessive disorder, caused by a mutation in the hemoglobin gene, and it follows the same 25 percent risk pattern as cystic fibrosis when two carriers have children. A person needs two copies of the sickle allele to develop the disease, while a person with one copy is a carrier, said to have sickle cell trait.
The twist that makes sickle cell remarkable is heterozygote advantage. Carriers of the sickle allele, who carry one normal and one sickle allele, gain partial protection against malaria. In regions where malaria is widespread, this protection gave carriers a survival edge, which kept the sickle allele common in those populations despite the harm of the homozygous disease. It is a striking example of how a disease allele can persist, even spread, when the carrier state offers a benefit. This shows that "recessive disease allele" does not always mean "purely harmful."
Sickle cell also illustrates a subtle point about dominance that depends on how you look at it. At the level of the disease, sickle cell behaves recessively, since two alleles are needed to be affected. At the molecular level, carriers produce both normal and sickle hemoglobin, which is a codominant relationship between the alleles. So the same condition can be described as recessive or codominant depending on whether you focus on the disease or the proteins, a nuance explored further in our guide to codominance examples. For predicting affected children, though, it follows the standard recessive 25 percent rule. Two parents who both have sickle cell trait face the same one-in-four chance of a child with the full disease that any pair of recessive carriers would, regardless of the molecular subtlety.
Reading Genetic Disorders in a Family Tree
Beyond single crosses, genetic counselors use family trees, called pedigrees, to identify inheritance patterns and estimate risk across generations. A few telltale signs distinguish the patterns, and learning them lets you read a family history at a glance.
Autosomal recessive disorders tend to skip generations and appear in children of unaffected parents, because carriers pass the allele silently until two carriers meet. The disorder often seems to come from nowhere, affecting a child whose parents and grandparents were all healthy. It strikes males and females equally, since the gene is not on a sex chromosome. Autosomal dominant disorders, by contrast, appear in every generation, since each affected person has an affected parent, and they too affect both sexes equally. An affected child almost always has an affected parent, with no skipping.
The presence or absence of skipped generations is therefore a quick diagnostic. A trait that vanishes for a generation and reappears suggests a recessive pattern with hidden carriers. A trait present in every generation suggests a dominant pattern. X-linked patterns add a sex bias on top, with conditions like hemophilia striking far more males than females. Combining these pedigree clues with Punnett square calculations is the everyday toolkit of genetic counseling, and it turns a family's history into actionable risk estimates.
Recessive vs Dominant Disorders at a Glance
Because the two autosomal patterns behave so differently, it helps to see them compared directly. The contrast explains why genetic counselors always start by asking which pattern a disorder follows before estimating any risk.
| Feature | Autosomal recessive | Autosomal dominant |
|---|---|---|
| Copies needed to be affected | Two | One |
| Carrier state | Yes, healthy carriers exist | No carriers |
| Risk from typical at-risk couple | 25% (two carriers) | 50% (one affected parent) |
| Pattern in family tree | Can skip generations | Appears every generation |
| Examples | Cystic fibrosis, sickle cell | Huntington's, Marfan syndrome |
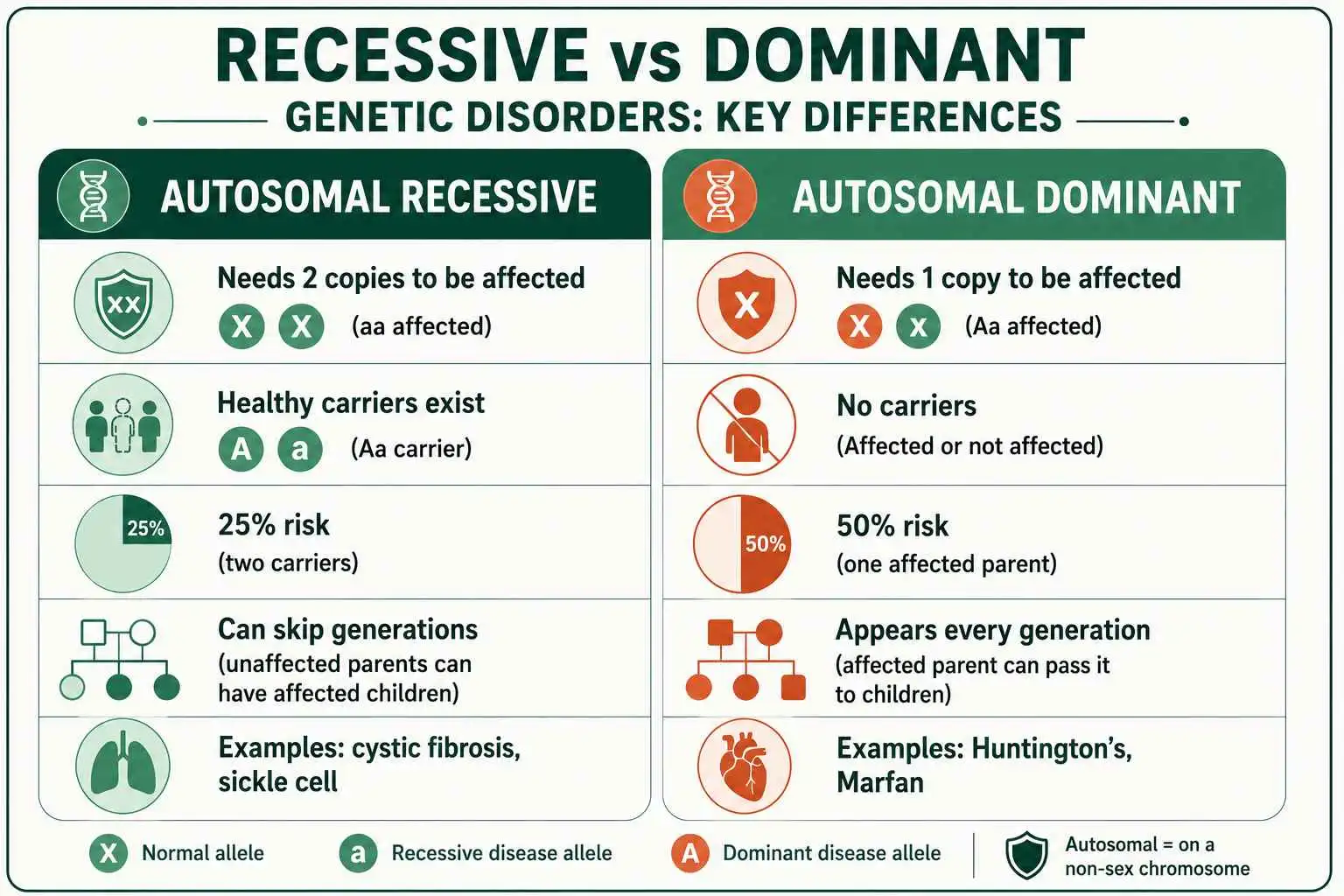
The table makes the practical difference clear. A recessive disorder hides in carriers and can surprise a family that has never seen it, while a dominant disorder is visible in each generation and carries a higher per-child risk. Neither pattern is simply worse than the other. Recessive disorders are easier to carry unknowingly, while dominant disorders are harder to escape once a parent is affected. As OpenStax notes, the same 3:1 Mendelian ratio that governs pea plants underlies the 25 percent recessive risk, which is a reminder that disease genetics rests on the same foundation as the classic crosses. Knowing where a disorder falls on this table is the fastest way to anticipate both its risk and its behavior across a family.
When the Simple Predictions Need Caveats
The clean 25 percent and 50 percent figures assume straightforward single-gene inheritance, but real genetics sometimes adds wrinkles. Knowing these caveats keeps a Punnett square prediction honest, especially for serious conditions where families deserve the full picture.
One important concept is penetrance, which describes how often people who carry a disease allele actually develop the condition. Some dominant disorders show incomplete penetrance, meaning a person can carry the allele yet never show symptoms, so the real-world risk can be lower than the Punnett square suggests. A related idea is variable expressivity, where the same allele produces mild symptoms in one person and severe symptoms in another. Both mean that carrying a disease allele does not always translate neatly into a predictable outcome, even when the inheritance pattern is clear.
New mutations add another layer. A child can occasionally develop a dominant disorder with no family history at all, because the disease allele arose fresh in that individual rather than being inherited. This is why a dominant condition sometimes appears to come from nowhere despite both parents being unaffected. Other complications include disorders influenced by multiple genes or by environmental factors, which a single-gene Punnett square cannot fully capture. None of this makes the Punnett square useless. It remains the right starting point for single-gene disorders, but these caveats explain why genetic counselors combine the basic math with detailed testing and family history rather than relying on the square alone. The prediction is a foundation, not the final word, and treating it that way is part of using it responsibly.
Why These Predictions Matter
The practical value of these Punnett square predictions is enormous, because they let families make informed decisions with real understanding rather than fear of the unknown. Genetic counseling exists precisely to translate inheritance patterns into clear, personalized risk information.
Carrier screening is one major application. Prospective parents can be tested to learn whether they carry alleles for common recessive disorders like cystic fibrosis or sickle cell. If both partners turn out to be carriers, they learn about the 25 percent risk to each child and can consider their options with full information. For dominant disorders like Huntington's, a person with an affected parent can choose whether to be tested for the allele, knowing each child faces a 50 percent risk if they carry it. These are deeply personal decisions, and accurate genetic information supports them.
The predictions also guide medical care. Knowing a child is at risk for a specific disorder allows for early monitoring, prenatal testing, or preparation for treatment. Newborn screening programs test for several genetic disorders precisely so that conditions can be managed early. In all these cases, the humble Punnett square, scaled up with modern genetic testing, is the foundation that turns the abstract rules of inheritance into concrete help for real families. The same probability principles that predict a pea plant's flower color carry genuine weight when the trait in question is a person's health.
Frequently Asked Questions
What is the chance of inheriting cystic fibrosis from two carrier parents?
There is a 25 percent chance. Each carrier parent has a 50 percent chance of passing the disease allele, so a child has a 50 percent times 50 percent, or 25 percent, chance of inheriting two copies and being affected. There is also a 50 percent chance the child is a carrier.
Why is Huntington's disease risk 50 percent?
Because Huntington's is caused by a dominant allele, a single copy causes the disease. An affected parent is usually heterozygous, so each child has a 50 percent chance of inheriting the disease allele, and anyone who inherits it will develop the condition since there is no carrier state.
What is the difference between a dominant and recessive genetic disorder?
A recessive disorder requires two copies of the disease allele to appear, so unaffected carriers exist and the disease can skip generations. A dominant disorder needs only one copy, so there are no healthy carriers and the condition appears in every generation.
Can a genetic disorder skip a generation?
Yes, autosomal recessive disorders commonly skip generations. The disease allele passes silently through healthy carriers and only appears when a child inherits two copies, which can be generations after the allele last caused symptoms in the family.
Key Points to Remember
Punnett squares turn genetic disorder risk into clear numbers once you know the inheritance pattern. Autosomal recessive disorders like cystic fibrosis and sickle cell require two disease alleles, so two carriers face a 25 percent risk per child and the condition can hide in healthy carriers for generations. Autosomal dominant disorders like Huntington's need only one allele, giving a 50 percent risk per child with an affected parent and no carrier state at all. The inheritance pattern sets both the odds and the way the disorder travels through a family.
These calculations are the backbone of genetic counseling, helping families understand carrier screening, prenatal testing, and their real risks. You can model any disorder cross and see the genotype and risk breakdown with the Punnett Square Calculator, keeping in mind that real genetic counseling combines this math with testing and professional guidance. For an authoritative medical reference on these inheritance patterns, this resource from StatPearls is a reliable place to read further.
This article covers genetic disorders for educational purposes. If you have personal concerns about inherited conditions in your family, a licensed genetic counselor or physician can provide guidance tailored to your situation, and is the right source for decisions about testing or care.